Cataract Lens (IOL) Options — Find the Best Fit for Your Vision
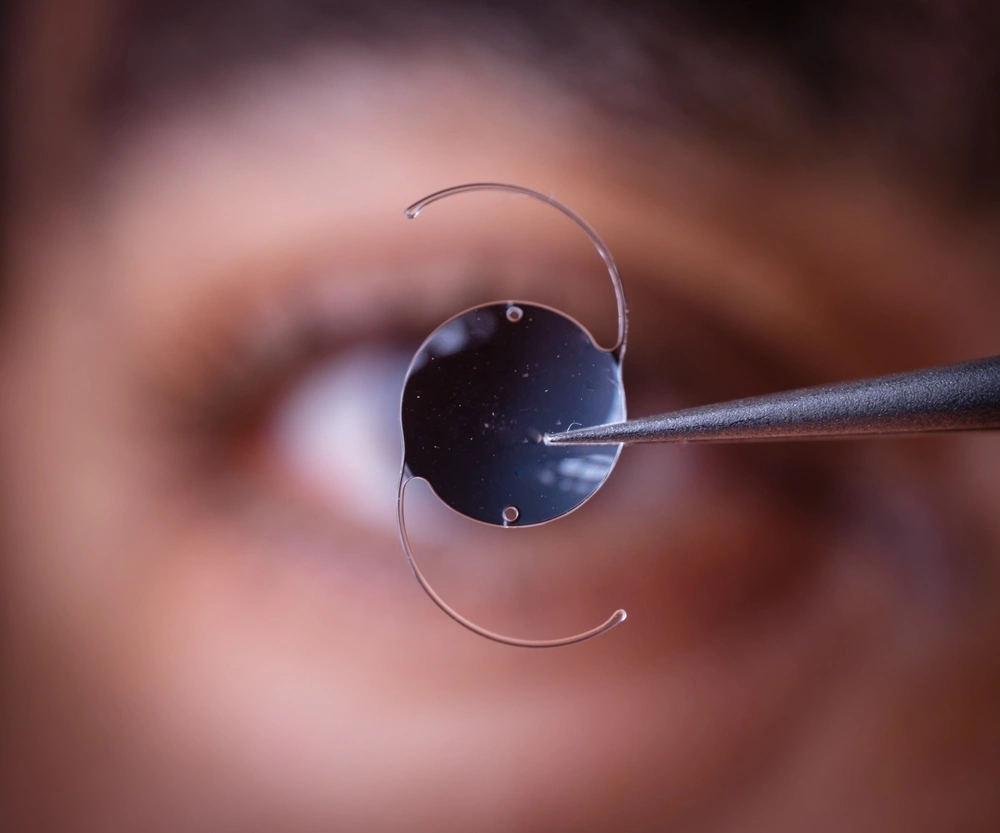
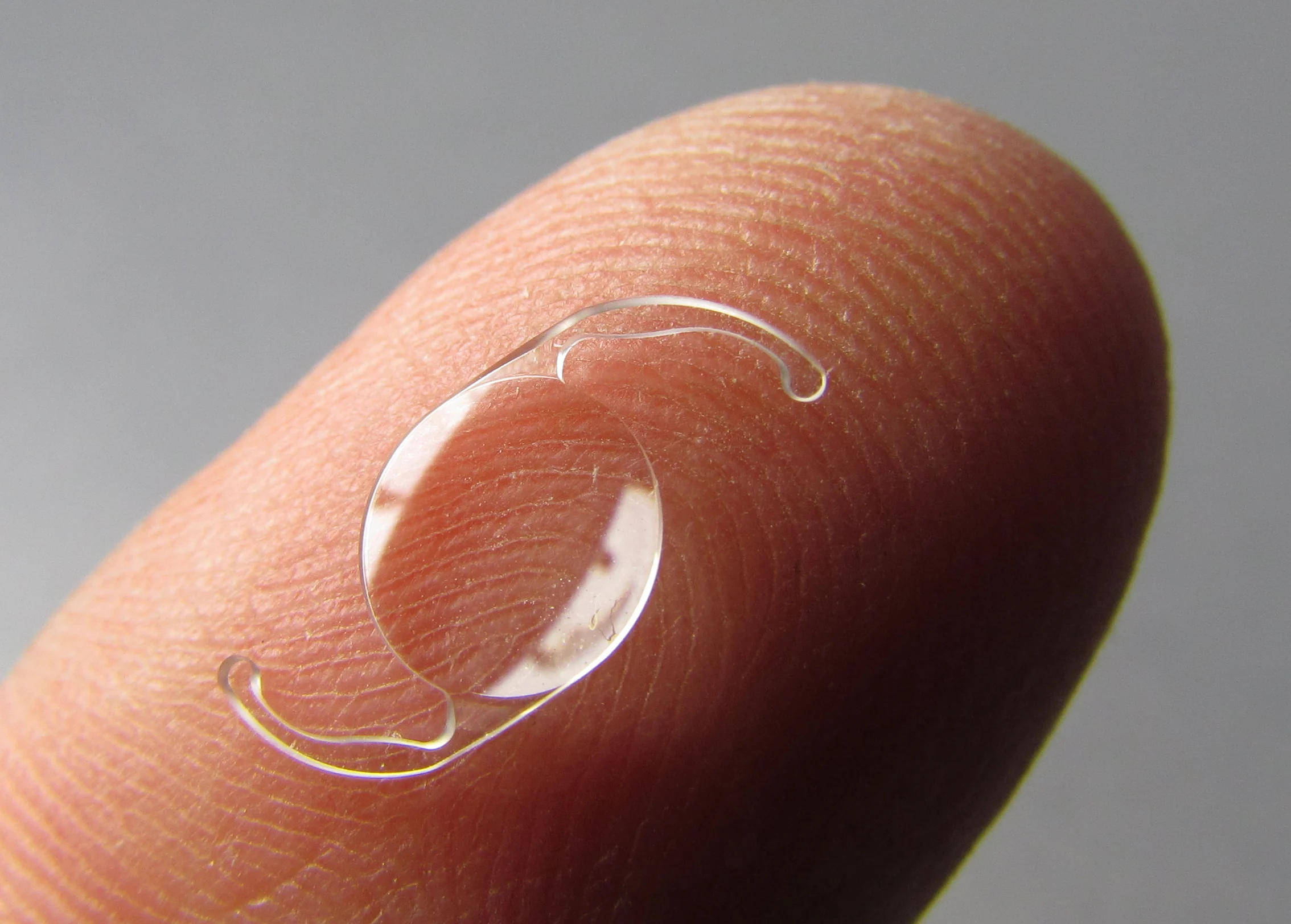
Cataract surgery replaces your cloudy lens with a clear intraocular lens (IOL). Choices vary in range of vision, night halos, contrast, and spectacle independence. We select together—based on your eyes, lifestyle, and medical safety.
Monofocal
Sharp distance (or near) in one focal range; highest contrast; reading glasses usually needed.
Advanced Monofocal (“enhanced”)
Similar safety/contrast to monofocal with better intermediate; some still need readers.
Toric (for astigmatism)
Any of the above with astigmatism correction; outcomes depend on rotation stability and precise alignment.
EDOF
Broader range to arm’s-length; fewer halos than trifocal but usually needs a light reader for fine print.
Trifocal
Distance + intermediate + near with highest spectacle independence; more halos/glare risk at night.
Book a cataract counseling session
Schedule your consultation with Dr. Praveen Saluja — begin your journey to clear vision.
“Best” = what fits your cornea, macula, occupation, night driving, dry eye, etc. Evidence shows trade-offs (range of vision vs photic phenomena/contrast).
Is there a ‘no-glasses guarantee’?
No—residual refractive error and neuroadaptation vary.
Toric IOLs — Cataract + Astigmatism Correction
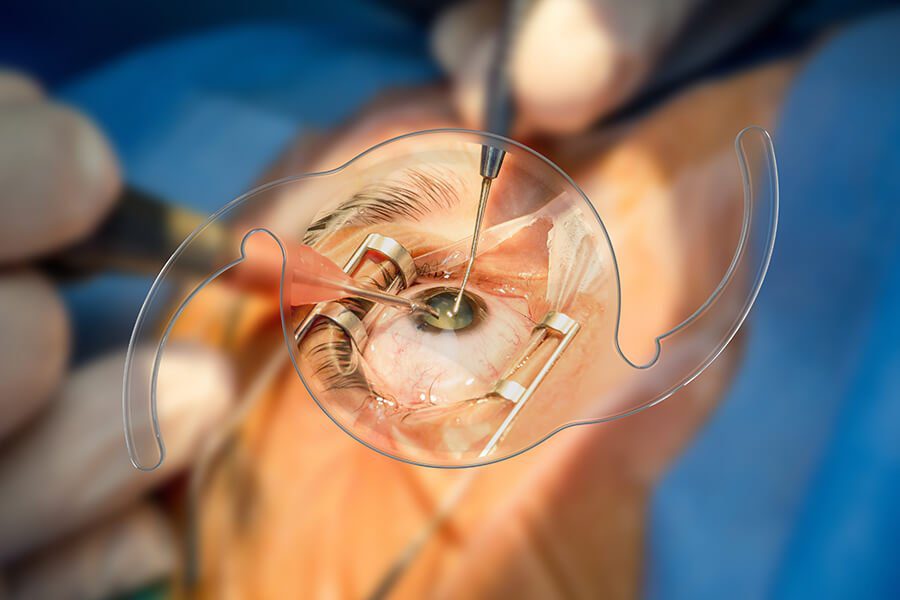
Corrects regular corneal astigmatism during cataract surgery. Outcomes depend on accurate axis alignment and post-op rotational stability.
Follow-up focus: Early rotation checks improve outcomes; re-alignment can restore intended vision if misaligned.
Who benefits?
Patients with ≥0.75–1.00 D corneal astigmatism.
What to expect:
Similar distance quality as monofocal when aligned; residual cylinder reduces sharpness.
Marking/IOP control, capsulorhexis sizing, and modern guidance systems are used for precision.
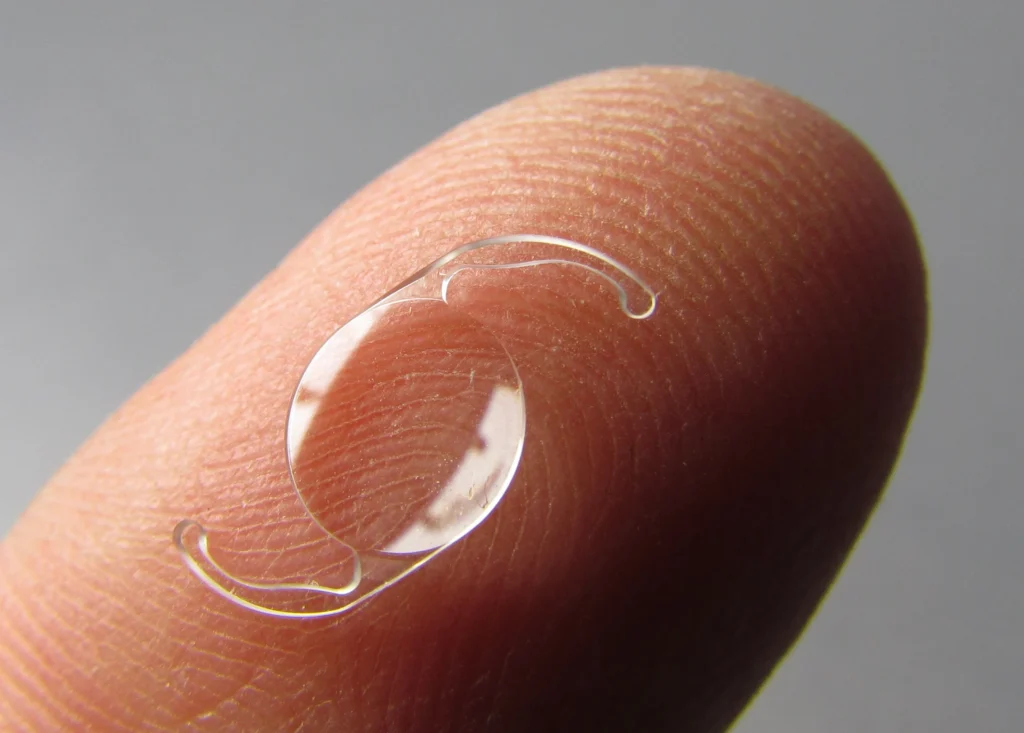
Monofocal IOL — Gold-Standard Safety and Clarity
Single focal point (usually distance); highest contrast and lowest night halos; readers usually needed.
Ideal when macular disease, glaucoma risk, or night-driving priority. (Conservative choice remains evidence-supported.)
Vision outcome
Excellent distance UCVA with refraction targeting.
Glasses expectation:
Reading and sometimes computer glasses.
Who should prefer:
Ocular comorbidities, professional drivers, pilots, or halo-averse patients.
Advanced (Enhanced) Monofocal — Extra Range for Daily Life
Preserves monofocal-like quality while boosting intermediate vision (dashboard/screen).
Lower photic phenomena vs diffractive designs; many still need readers for fine print.
When ideal:
Office/computer users; halo-averse; early presbyopes.
Evidence snapshot:
Enhanced IOLs improve INT/Near vs conventional monofocals; more data emerging on contrast/QoV.
EDOF IOL — Wider Range, Natural Night Vision Profile
Extends depth of focus for distance + intermediate and some near; typically fewer halos than trifocal but more than monofocal.
Different platforms (diffractive vs refractive) show good distance, stronger intermediate, and variable near; contrast generally between monofocal and trifocal.
Ideal profiles:
Professionals needing screens, active drivers at night, willing to use thin readers for fine print.
Evidence snapshot:
Multiple 2024–2025 reports show better INT/near than enhanced monofocal and high satisfaction; residual Rx tolerance improving in newer refractive EDOF.
Trifocal IOL — Distance, Intermediate & Near with Max Spectacle Independence
Highest chance of glasses-free across ranges; trade-off is more halos/glare and potential contrast reduction, especially in low light.
Neuroadaptation usually improves symptoms over weeks to months. Comparative analyses show very high satisfaction despite more photic phenomena.
Who should consider:
Strong desire for near independence, minimal ocular comorbidity, realistic night-driving expectations.